
Lung cancer is one of the deadliest types of cancer in the world – often undetected for a long time, socially stigmatized and emotionally distressing. However, it is precisely with this disease that medical research has made tremendous advances in recent years. These breakthroughs were made possible by targeted investments in oncology – with major involvement from research-based pharmaceutical companies in Switzerland.
From death sentence to hope for time and quality of life
Until the mid-20th century, lung cancer was considered a rare disease. It was only with the high prevalence of smoking that the number of cases skyrocketed – first among men and later, with a time lag, among women1. Today, lung cancer is one of the most common types of cancer in the world and is also the leading cause of cancer-related death. In Switzerland, around 4,900 people develop the disease every year, most of them in later life2.
Until the 1990s, lung cancer was usually only diagnosed at an advanced stage – often with metastatic tumors and a relatively poor prognosis. For a long time, the five-year survival rate was below 10%3. Since then, and thanks to advances in diagnostics and a new generation of targeted and cancer immunotherapies, treatment options have significantly improved. As of 2024, the five-year survival rate for those affected has risen to 30%3.
This change was largely due to the realization that lung cancer is not a homogenous disease. Classification into small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC) – the latter accounting for about 85% of cases – now forms the basis for the choice of therapy4. Targeted treatment has significantly improved the prognosis for many patients – while at the same time being better tolerated than conventional therapies.
Smoking remains by far the biggest risk factor. Other influences such as air pollution, occupational exposure to carcinogens (e.g. asbestos) and genetic predisposition play a complementary role – particularly in non-smokers and younger patients1.
Research saves lives: the path to modern therapy
For decades, conventional therapy consisted of surgery, radiotherapy and non-specific chemotherapy, often with significant side effects. The turnaround came with a better molecular understanding of tumor biology. Researchers discovered mutations and growth factors as the cause of cancer and began to develop targeted therapies. Today, targeted therapies (such as EGFR, ALK and ROS1 inhibitors) and immunotherapies that activate the immune system to detect and destroy cancer cells are available5. One milestone was the approval of the first checkpoint inhibitors, which can significantly prolong survival in certain patient groups – with significantly better tolerability than conventional cytostatic drugs used in the context of chemotherapy.
Switzerland – an innovation hub in oncology
Although research into lung cancer is global, Switzerland plays a key role. Strong basic research and the networking of all research stakeholders is essential to Switzerland’s success. International studies are conducted in Swiss clinics and pharmaceutical companies from all over Switzerland are directly involved in developing new active substances. Switzerland is one of the leading countries in clinical research in oncology – with a high participation rate in studies and rapid implementation in healthcare6. More than 70 oncological drugs are currently being developed for lung cancer – and many of them with Swiss participation7. The research aims to make therapies not only more effective, but also more tolerable and targeted.
Universities, hospitals and the industry are working closely together to advance biomarker-based diagnostics and precision medical therapies. One example is the combination of immunotherapy and chemotherapy, which is now considered the standard treatment for advanced non-small cell lung cancer – with good results in selected patient groups5.
Rethinking lung cancer: precision instead of standardized treatment
Lung cancer has long been regarded as a disease that is difficult to treat, but this picture is increasingly changing due to modern diagnostics and targeted approaches to treatment. Today, the focus is no longer on the type of disease alone, but on the individual tumor profile. What genetic changes drive the growth? Which immune response can be activated?
This personalized approach – supported by molecular tests – allows targeted therapies with improved efficacy and higher tolerability. What used to be treated uniformly with chemotherapy is now viewed in a nuanced way – and is increasingly being treated successfully.
1 Goeckenjan G.: Lung cancer – historical development, current status, future prospects – https://www.thieme-connect.com/products/ejournals/pdf/10.1055/s-0030-1255636.pdf
2 Federal Statistical Office (FSO): Swiss health statistics
3 Swiss Cancer League: lung cancer statistics 2023 – www.krebsliga.ch
4 American Cancer Society: types of lung cancer – www.cancer.org
5 Swiss Cancer Research Foundation: Oncology in transition – 2022 annual report
6 Interpharma: Research for a healthier future – 2023 report
7 Pharmaceutical Research and Manufacturers of America (PhRMA): Medicines in development – oncology 2023
Researchers have only been aware of the link between human papillomaviruses (HPV) and various types of cancer for the past few decades. Today, we know that certain types of HPV are primarily responsible for the development of cervical cancer and other tumors in the genital and head and neck area. Since then, medical advances have yielded remarkable results. Vaccines, new screening methods and innovative treatments are proving effective in preventing or treating HPV infections and their serious consequences at an early stage.
A human papillomavirus (HPV) infection can have life-changing consequences. Even so, most people do not notice anything at first, as many HPV infections heal spontaneously. However, some remain – and years later can cause serious illnesses such as cervical cancer, rectal cancer or throat cancer.
In Switzerland, around 250 new cases of cervical cancer are diagnosed every year and around 70 women die from it1. This type of cancer claims hundreds of thousands of lives worldwide2. Many of these tragedies could be prevented thanks to the effective options offered by research and medicine today: vaccination, early detection and innovative treatments.
What are human papillomaviruses (HPV)?
HPV is a group of more than 200 different virus types. Of these, around 40 affect the mucous membranes of the genital area and other regions. Some types cause benign genital warts. Others, known as high-risk HPV, can lead to cancer2.
HPV is primarily transmitted through sexual contact. It is estimated that more than 80% of sexually active people will become infected with HPV at least once in their lives [2]. In most cases, the infection has no consequences – but for a small group of individuals it can have serious consequences.
From threat to opportunity: milestones in HPV research
Just a few decades ago, the link between HPV and cancer was all but unheard of. Women with cervical cancer often received a poor prognosis. Thanks to groundbreaking research, it is now clear that almost all cases of cervical cancer are due to chronic infection with high-risk HPV2.
This breakthrough was the basis for the development of HPV vaccines. These vaccines have been available since 2006 and provide targeted protection against the most dangerous types of human papillomavirus. New generations of these vaccines now cover even more virus types, thus offering further protection2.
Great strides have also been made in the field of early detection. The classic Pap smear has been supplemented by modern HPV tests that can detect infections at a much earlier stage – even before pathological cell changes or the development of cancer4.
At the same time, research into treatments is progressing steadily: researchers are working on innovative forms of immunotherapy that can be used specifically against existing HPV-associated tumors6.
Vaccination: a triumph of prevention
The HPV vaccines mentioned above are now a key component of prevention. They prevent infections involving the most dangerous HPV types – and therefore most cases of cervical cancer3. In Switzerland, vaccination is recommended for all male and female adolescents aged 11 to 141. Booster vaccinations can be given up to the age of 26. In regions with high vaccination rates, the incidence of precancerous diseases has already fallen by up to 88%3.
In addition to the widespread use of proven vaccines, research into new, even more targeted approaches is progressing steadily. An impressive example of this progress is a vaccine candidate that specifically targets HPV-16-positive tumors. Initial studies show a significant improvement in the survival rate among patients with advanced cervical or head and neck cancer6. Further research is now also being conducted into mRNA technology, which became known worldwide due to COVID-19, for use in HPV vaccines and treatments3.
Early detection: stopping cancer before it develops
Medicine offers protection even if an infection has already occurred: regular HPV tests and Pap smears allow cell changes to be detected at an early stage. Modern tests are more sensitive than traditional methods and allow for even more targeted prevention4. In Switzerland, women between the ages of 21 and 70 are offered screenings1. Recent recommendations discuss the use of HPV primary tests, which test directly for viral infections rather than cellular changes. Initial studies suggest that this could further improve the detection rate3.
New horizons: treatments of the future
Research does not end with prevention. Researchers are currently developing promising therapies for the treatment of existing HPV-associated cancers. The focus is on a variety of innovative approaches. Immunotherapies aim to activate the body’s own immune system against HPV-positive tumor cells6. In addition, therapeutic vaccines are being researched that do not protect against infection like conventional vaccines, but counteract existing HPV infections and the resulting cancers. Gene therapies, which can repair or deliberately destroy diseased cells, are also opening up new treatment paths. Personalized immunotherapies that are individually tailored to the genetic and molecular characteristics of a tumor are a particularly exciting development. These promising approaches are currently in the clinical trial stage and could play an important role in cancer treatment in the future6.
Research for an HPV-free future in Switzerland
Switzerland is heavily involved in the fight against HPV. National vaccination programs, education campaigns and scientific projects such as the “Swiss HPV Vaccination and Screening Program” are proof that research, politics and society can make progress together1. As a home to many innovative biotech and pharmaceutical companies, Switzerland invests billions into medical research every year. Projects involving the development of new vaccines or treatments against HPV benefit from this dynamic environment.
1 Federal Office of Public Health (FOPH). HPV Information, 2023.
2 WHO. Global strategy to accelerate the elimination of cervical cancer, 2022.
3 Lancet. Population-level impact and herd effects following human papillomavirus vaccination programmes: a systematic review and meta-analysis, 2021.
4 Swiss Cancer League. Cervical cancer and HPV.
5 Gavi, the Vaccine Alliance. HPV Vaccine Programmes, 2023.
6 De Vos van Steenwijk PJ et al. ISA101 and immune-checkpoint blockade: a phase 2 study. Lancet Oncol. 2019.
Evidence of excessive body weight can already be found in ancient writings – but the cause remained unclear for millennia. For a long time, being overweight was seen as a lack of discipline. Those who suffered from the condition were ridiculed or ostracized. It was not until the 20th century that medicine began to recognize obesity for what it is: a complex, chronic disease with multiple causes1.
First scientific milestones
In the 19th century, researchers first discovered correlations between metabolism, hormones and body weight. For a long time, however, there was a lack of understanding of the complex mechanisms in the human body. A genuine breakthrough finally came in 1994:
The discovery of the hormone leptin – a neurotransmitter that regulates the body’s fat reserves via the feeling of hunger – marked a turning point2.
Further research revealed that not only leptin, but also hormones such as ghrelin and GLP-1, play a key role in controlling hunger and satiety3. These findings fundamentally changed the understanding of obesity: The disease was no longer regarded merely as the consequence of a weak will, but as a medical problem.
A new approach via hormone-based therapies
While diet and exercise used to be the only treatment options, the discovery of GLP-1 receptor agonists revolutionized the treatment of obesity. These are medications that specifically intervene in the hormonal control of appetite. They mimic the effect of the natural intestinal hormone GLP-1, which is secreted after eating and signals to the body that it is full,
thereby reducing the feeling of hunger and lowering food intake. Originally developed to control blood sugar levels in type 2 diabetes, it soon became apparent that these active substances not only influence sugar metabolism, but also eating habits4.
By increasing their natural feeling of satiety and slowing gastric emptying, patients were able to significantly and sustainably reduce their weight – a breakthrough that for the first time offered hope in a drug treatment for obesity.
Medical advances make their way into everyday life
In Switzerland, the new therapies were introduced step-by-step. Swissmedic approved the first active substances for weight loss back in 2016. These caused an average weight reduction of 15 to 20% – an order of magnitude previously only achievable with surgical procedures4. They also significantly reduce the risk of concomitant diseases such as diabetes, heart attack and certain types of cancer3.
Compulsory health insurance in Switzerland recently, and under strict conditions, began covering the costs of these treatments – marking a milestone in patient care5.
A glimpse into the future
Research, however, is not at a standstill. New combination therapies, such as GLP-1/GIP dual agonists, show even better results in studies, with patients losing up to 22% of their body weight [6]. In the future, precision medicine – based on genetic, metabolic and individual profiles – could make treatment even more targeted and effective3.
Innovations such as orally administered GLP-1 therapies or implantable systems for continuous release of the active substance are already in the development stage.
Social change through medical research
What used to be perceived primarily as a personal failure is now being re-evaluated. Medical advances have permanently changed the picture of obesity, away from a stigma towards an acknowledged chronic disease that is treatable.
For the millions of people affected this not only results in better health, but also improves quality of life and participation in society. At the same time, successful therapies also relieve the burden on healthcare systems in the long term by reducing secondary diseases and the associated costs1. We keep researching.
1 Federal Statistical Office (FSO). Body weight and health in Switzerland. Neuchâtel, 2022.
2 Friedman JM, Halaas JL. Leptin and the regulation of body weight in mammals. Nature. 1998.
3 Müller TD et al. Obesity pharmacotherapy: what we have, what we need, and what’s next. Nat Rev Drug Discov. 2022.
4 Wilding JPH et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021.
5 Swissmedic. Product information Saxenda® and Wegovy®.
6Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022.
Migraine was long a medical mystery. Millions of people suffered – often in silence, and frequently misunderstood. As migraine sufferers know all too well, it often comes on suddenly, with full force. The day starts off normally, but a just few hours later the head is pounding and throbbing. What sounds like a “severe headache” to outsiders is a serious neurological crisis for those affected.
A glimpse into the past – from myths to molecules
The oldest texts describing migraine-like symptoms go back to 3,000 BCE.
In old Europe, it was long believed that migraine was caused by “rising vapors” in the brain. The thinking slowly began to change in the 17th century. British doctor Thomas Willis recognized that migraine probably had something to do with the blood vessels – a decisive step towards modern therapeutic approaches.
An illness with serious consequences
Today, migraine is recognized as one of the most common neurological disorders worldwide. Around one million people in Switzerland – roughly one in seven to ten people – suffer from it. Women are three times more likely to be affected than men1. Despite its prevalence, migraine was neglected as a field of scientific inquiry for decades. It was only in recent times that modern research enabled key advances in understanding the causes of the disease, with positive consequences for treatment and the quality of life of those affected.
A migraine attack is not a “normal” headache. It is an expression of highly sensitive stimulus processing in the brain. Around a quarter of patients also experience what is known as an aura, which is characterized by visual disturbances, numbness, speech problems or dizziness. These attacks can last for many hours or even days and completely shut down everyday life. In Europe alone, migraine causes billions of dollars in economic damage every year, mainly through missed work and lost productivity3.
New insights through modern research
Migraine was long regarded as a purely vascular disorder – a view that was reflected in the standard therapies of the second half of the 20th century. Earlier medications therefore focused primarily on narrowing the blood vessels. But there was a real breakthrough in the 1980s with the discovery of what is known as the trigeminovascular system. Researchers discovered that a nerve plexus in the brain interacts closely with the blood vessels of the meninges4.
At the heart of this network is a neurotransmitter that is released during a migraine attack and triggers an inflammatory response in the brain tissue. This central mechanism is now considered the main cause of typical migraine pain5. This new insight not only changed research, but also revolutionized therapy.
Drugs with a targeted effect
These findings made it possible to develop a drug therapy that specifically intervenes in the biological processes of migraine. Triptans came onto the market in the 1990s. They inhibit the release of the neurotransmitter while at the same time constricting the dilated blood vessels. Many patients benefited from this new group of medications. Triptans proved not to be suitable for everyone, however. There are limitations for people with cardiovascular diseases6 in particular.
Researchers therefore sought alternative mechanisms of action, which led to the development of gepants. Gepants block receptors directly and have an anti-inflammatory effect without the vascular constriction. They are regarded as well tolerated and can also be used for prevention7.
Antibody therapy marked another milestone. It enables a long-term reduction in the frequency of migraine attacks; in many cases, one injection per month is sufficient. Clinical studies have shown significant improvements in the quality of life of people with chronic migraine8.
Innovations on the horizon – what the future holds
Research into migraine continues apace. Work is now underway on personalized therapeutic approaches that are tailored to the genetic characteristics of the individual patients. The aim is not only to provide better treatment, but also to precisely tailor the therapies9. New non-drug approaches are also being developed, including therapies in which electric or magnetic impulses target regions of the brain that are involved in the development of migraines10.
Even the color of light is being studied. Initial clinical studies indicate that a green light can reduce the intensity of migraine pain in some patients11. Digital technologies are also increasingly being used in treatment, with migraine apps that document attacks and analyze progression patterns, thus helping to better recognize individual triggers and adapt therapies12.
Research changes lives
The history of migraine is an impressive example of how medical research leads to real progress. What was a mystery for centuries is now understood – and treated effectively. Millions of people benefit from targeted, modern medicines, improved diagnostic procedures and a new medical understanding of the disease. This transformation is the result of decades of research. Interpharma is dedicated to ensuring that this path of advancement continues. After all, progress requires scientific curiosity and a clear vision: the mission of treating migraines effectively. We keep researching.
1 Federal Office of Public Health (FOPH). Swiss headache and migraine statistics.
2 Ashina M. Migraine. New England Journal of Medicine. 2020;383(19):1866–76.
3 Lanteri-Minet M et al. Economic impact of migraine. Cephalalgia. 2011;31(8):867–79.
4 Goadsby PJ et al. Pathophysiology of migraine: a disorder of sensory processing. Physiological Reviews. 2017;97(2):553–622.
5 Edvinsson L. The CGRP pathway in migraine as a viable target for therapies. Headache. 2018;58(S1):33–47.
6 Tfelt-Hansen P, Olesen J. Taking the negative view of current migraine treatments. Headache. 2012;52(7):1159–65.
7 Dodick DW et al. Ubrogepant for the acute treatment of migraine. New England Journal of Medicine. 2019;381(23):2230–41.
8 Tepper S et al. Efficacy and safety of erenumab for preventive treatment of chronic migraine. Lancet Neurology. 2017;16(6):425–34.
9 Borsook D et al. Personalized medicine for migraine: an evolving landscape. Headache. 2021;61(5):725–35.
10 Chou DE et al. Noninvasive neuromodulation for migraine. JAMA Neurology. 2017;74(5):571–6.
11 Noseda R et al. A human fMRI study on green light and photophobia. Brain. 2016;139(Pt 7):1971–80.
12 Schwedt TJ et al. Use of smartphone technology in the management of migraine. Headache. 2019;59(6):802–16.
The symptoms of hepatitis were first described as early as the 5th century BCE. However, nobody knew where hepatitis came from or how to treat it at that time. Today effective vaccinations offer protection against hepatitis A and B. Although there is still no vaccination against hepatitis C, the chances of recovery are over 95% thanks to modern treatments.1
Unidentified for centuries
Reports of outbreaks of epidemic jaundice, a common consequence of hepatitis, date back to ancient times. However, it was not until the mid-20th century that it was discovered that hepatitis is mostly caused by viruses. In 1947, the British physician F.O. McCallum first made the distinction between hepatitis viruses A and B. In the late 1980s, researchers finally discovered the hepatitis C virus, which is often chronic and therefore considered the most dangerous hepatitis virus. An estimated 400 million people worldwide are infected with one of the virus variants, and over 1.3 million people die from the disease every year.2
Hepatitis can be treacherous because many symptoms occur gradually. It can often take years before those affected notice that they have been infected – with serious consequences for the liver.
Breakthrough vaccination against hepatitis
hepatitis A and B (also available as combination vaccine). The first hepatitis A vaccines were approved in Europe in 1991. They are now on the World Health Organization (WHO) List of Essential Medicines, as they offer protection against one of the most common infectious diseases in high-risk regions such as Africa, Asia, Central America and South America with an effectiveness rate of 95–99%. Vaccination is therefore recommended for all travelers visiting a country with a high prevalence of hepatitis A.3
Vaccination against the hepatitis B virus has been available since 1984. It is one of the primary vaccines in Switzerland and offers vaccinated people 10 years of immunity – with a booster in adulthood, this immunity even lasts for decades.4 The vaccination recommendation for adolescents, which the Federal Office of Public Health (FOPH) introduced in Switzerland in 1998,5 has significantly contributed to the steady decline in the number of new hepatitis B infections in Switzerland:
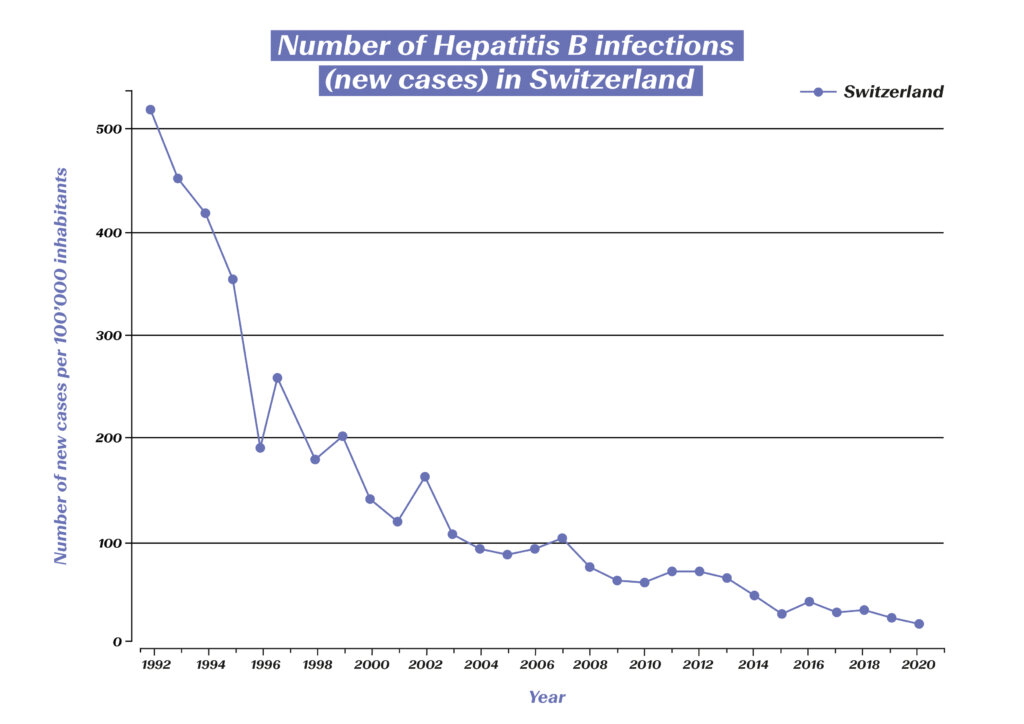
Number of hepatitis B infections (new cases) in Switzerland. (Source: Statista) https://de.statista.com/statistik/daten/studie/544724/umfrage/neuerkrankungen-an-hepatitis-b-in-der-schweiz/
Thanks to the high rate of immunization, the estimated global prevalence in children under the age of five has been reduced from 4.7% to below 1% over the past 40 years. Studies also show a threefold lower incidence of liver cancer caused by this virus variant among vaccinated people. The hepatitis B vaccine could therefore even be described as a vaccination against cancer.4
Advances in treatment thanks to targeted research
If infection with a hepatitis virus occurs and becomes chronic, this can have serious consequences and may lead to liver cirrhosis or liver cancer. While hepatitis A never becomes chronic, this can happen with both hepatitis B and C. Thanks to new developments in medical research, however, chronic disease can now be treated effectively.
In the event of a hepatitis B infection, antiviral agents are used which reduce the viral load in the blood, thereby preventing serious complications. In addition, new virological diagnostic methods are making it increasingly easy to determine the best treatment option.
Treatment of hepatitis C has come a long way since the virus was discovered in 1989. At first, patients were treated with interferons for six to 12 months. The cure rate was initially less than 20%, and involved considerable side effects for the patients. In the second decade, the cure rate was gradually increased to 45%, in part through the combination with ribavirin. Decisive progress has finally been made in the last two decades – the identification of the protein structure enabled the development of highly potent antiviral drugs with an excellent safety profile. In 2015, a breakthrough in cure rates and side effects was finally achieved with interferon-free treatment.6 Until recently, chronic hepatitis C was the most common cause of liver transplantation in Switzerland, but now 98% of all infections can be cured. On average, affected individuals are now virus free after just 8–12 weeks of treatment. As of 2022, all medications for the treatment of hepatitis C can be prescribed by doctors without restrictions.7 The treatments that have emerged through the power of biomedical research are now presenting a prospect long thought impossible: the global eradication of hepatitis C and thus of millions of human lives saved.
The WHO has therefore set itself the goal of global hepatitis B and C containment by 2030. The plan is to achieve this through a combination of different measures, but vaccines are the key to success. It can be expected that the rapid progress made in the development of COVID-19 vaccines will also boost the development of a vaccine against hepatitis C.8 Also, intensive research continues into even more effective treatment options for hepatitis B. In addition, the development of diagnostics continues to play a key role in the global fight against hepatitis.
1 Deutsches Bundesministerium für Bildung und Forschung (2019): Hepatitis – Eine unterschätzte Krankheit. https://www.gesundheitsforschung-bmbf.de/de/hepatitis-eine-unterschatzte-krankheit-mit-hoher-dunkelziffer-9689.php
2 Hepatitis Schweiz (2022): Was ist Hepatitis? https://hepatitis-schweiz.ch/formen/was-ist-hepatitis
3 Robert Koch Institut (2019): Hepatitis A. https://www.rki.de/DE/Content/Infekt/EpidBull/Merkblaetter/Ratgeber_HepatitisA.html
4 Gerlich, Wolfram H. (2022): Hepatitis-B-Impfstoffe – Geschichte, Erfolge, Herausforderungen und Perspektiven. Bundesgesundheitsblatt 65: 170–182.
5 Bundesamt für Gesundheit (2020): Impfungen – Zahlen und Fakten. https://www.bag.admin.ch/bag/de/home/strategie-und-politik/nationale-gesundheitsstrategien/nationale-strategie-impfungen-nsi/zahlen-fakten.html#:~:text=Schweizweit%20sind%2070%20Prozent%20der,von%2012%20bis%2089%20Prozent
6 Grätzel, Philipp (2019): Die Interferontherapie ist Geschichte. 13th Expert Summit on Viral Hepatitis, 10./11. Februar 2017, Berlin (Veranstalter: MSD). https://link.springer.com/content/pdf/10.1007/s15006-017-9415-x.pdf?pdf=button
7 Hepatitis Schweiz (2022): Neu können Hepatitis-C-Medikamente auch von Hausärzt:innen verschrieben werden. https://hepatitis-schweiz.ch/news/neu-koennen-hepatitis-c-medikamente-auch-von-hausaerztinnen-verschrieben-werden
8 Swiss Medical Forum (2022): Hepatitis C ist heilbar: eine Erfolgsgeschichte der biomedizinischen Forschung. https://medicalforum.ch/de/detail/doi/smf.2022.09003
Early diagnosis and prompt, appropriate treatment are the key to successfully dealing with rheumatoid arthritis (RA). The widespread inflammatory joint disease has been around for thousands of years – but breakthroughs were only made in the 20th century. The disease can now be managed so well in more and more affected individuals that they can live with almost no symptoms.
Millennia-old bone finds and famous patients – the history of RA
Bone finds have shown that rheumatoid arthritis (RA) was around as early as 4500 BC. From then on, texts often mention diseases with symptoms matching those of RA. A famous patient in the 17th century was the Flemish painter Rubens, who often depicted hands with rheumatism in his later works. In 1859, the British doctor Alfred Baring Garrod introduced the term “rheumatoid arthritis” for the first time. At that time, treatments were limited to home remedies such as leech therapy. Medicines containing opiates and alcohol were later given to patients to provide some relief.
In the early 20th century, advances in radiology allowed RA to be more accurately diagnosed and differentiated from related conditions such as osteoarthritis. This marked the beginning of the era of modern approaches to RA – in 1941, the American Rheumatism Association recognized RA as a disease in its own right.
As with many diseases, gold was also used for RA from the 1920s. Gold salt injections, which only develop an effect after six months, are considered to be the first generation of base medication against RA. The base medications are also called DMARDs (disease-modifying antirheumatic drugs). These show anti-inflammatory action and are therefore suitable for long-term administration in patients constantly affected by inflammation.
The year 1948 is considered a key year for rheumatology in the 20th century. In the USA, Philipp S. Hench was the first to use cortisone to treat RA. This approach changed not only rheumatology, but also medicine as a whole, thereby improving the lives of countless patients. Various synthetically produced DMARDs were ultimately approved in the 1950s, such as hydroxychloroquine, which was originally used as an antimalarial agent.
Breakthroughs in the second half of the 20th century
The 1960s and 70s were primarily characterized by new diagnostic developments, which enabled a differentiated classification of various rheumatic diseases. Further milestones in the treatment of RA followed in the 80s and 90s. Among other things, a special highlight was the development of methotrexate. As one of the synthetically produced DMARDs, the medication was adopted quickly and widely in the 80s for its targeted anti-inflammatory effects, ushering in a whole new era of RA treatment.
At the end of the 20th century, the focus was placed on the development of biologic agents. These substances interfere with the inflammatory process, for example by neutralizing proteins that transmit inflammatory signals. Biologic agents include TNF-alpha inhibitors. These drugs are characterized by their outstanding effectiveness – better response rates were achieved in patients than ever before. In the years that followed, there were various new and further developments in the field of biologic agents. These breakthroughs brought with them the hope of slower disease progression or even remission (meaning a symptom-free state defined according to certain criteria) for increasing numbers of patients.
This rapid development has also continued in the last two decades. New modes of action were identified, and corresponding medicines brought onto the market (e.g. anti-IL-6 receptor antibodies and anti-CD20 antibodies in the field of biological agents as well as JAK inhibitors from the group of synthetic basie medications). In addition, new findings allowed the strategy for the use of cortisone medications to be adapted. These continue to play a key role but can now often be administered in smaller doses.1
Thanks to breakthroughs achieved via continuous research and development, a wide range of medicines is now available. This is highly significant since the course of RA differs between patient and the appropriate treatment must therefore be determined individually. Classic pain medications (analgesics), non-steroidal anti-inflammatory drugs (NSAIDs) for pain relief and anti-inflammatory effects, and cortisone products with a strong anti-inflammatory effect are used for the treatment of RA today. The medications from these groups bring great relief to patients, but have no impact on the course of the disease. DMARDs, on the other hand, do not relieve pain, but have an anti-inflammatory effect in a wide variety of forms (conventional or synthetically produced in a targeted manner or in the form of biological agents).2
However, if RA patients are not optimally treated with medication according to the latest knowledge, they will have a shorter life expectancy, as untreated RA can also spread to organs.3 Thanks to modern RA treatment, however, it has been possible to continuously reduce the number of RA-related deaths:

RA-related deaths among 50–69-year-old women in Switzerland (source: Global Burden of Disease (GBD), https://vizhub.healthdata.org/gbd-compare/#)

RA-related deaths among 70+-year-old women in Switzerland (source: Global Burden of Disease (GBD), https://vizhub.healthdata.org/gbd-compare/#
Precision medicine: fast diagnosis and minimizing the disease burden
The medical breakthroughs of recent years have brought enormous relief for affected patients and massively reduced the disease burden. For example, data from almost 40,000 patients in Germany points to a significant reduction in the mean disease burden. The proportion of those affected with low disease activity rose to almost 50% in the reviewed period. Optimized control of the disease even has an impact on socio-economic factors: at the end of the reviewed period, the number of sick days was almost three times lower than at the beginning.4
It is estimated that about 70% of all RA sufferers could theoretically achieve remission within the first year after diagnosis. In order to achieve this high level, early diagnosis and implementation of the correct treatment are essential.5 The availability of many different medications with differing modes of action allows for treatment adjustment where necessary until the treatment objective is achieved. With a combination of the correct medication and aid measures such as physiotherapy, symptoms can be minimized and the quality of life maintained accordingly.
Precision medicine is likely to provide further advances in the treatment of rheumatoid arthritis in coming years. Genetic analyses of joint tissue, for example, will make it possible to quickly predict which medications a patient will respond to. Patients will soon no longer be divided into different groups based on clinical parameters to predict the effectiveness of medications. Instead, individual genetic signatures will enable the development of tailored treatment regimens.6 Complications from progressive RA could therefore soon be a thing of the past.
1 Manger B. et al. (2020): 80 Meilensteine der Rheumatologie aus 80 Jahren. I-IV. Z Rheumatol.
2 Rheumaliga Schweiz (2021): Medikamente bei entzündlichem Rheuma.
3 Internisten im Netz (2017): Rheumatoide Arthritis: Prognose & Verlauf. https://www.internisten-im-netz.de/krankheiten/rheumatoide-arthritis/prognose-verlauf/#:~:text=Patienten%20mit%20rheumatoider%20Arthritis%2C%20die,um%203%2D13%20Jahre%20geringer
4 Fiehn, C. (2011): Rheumatoide Arthritis – Meilensteine für Klassifikation und Therapie. Dtsch Med Wochenschr 136: 203–205.
5 Deutsche Rheuma-Liga (2021): Rheumatische Erkrankungen: Zeit ist Remission. https://www.rheuma-liga.de/aktuelles/detailansicht/rheumatische-erkrankungen-zeit-ist-remission#:~:text=Theoretisch%20k%C3%B6nnten%20bis%20zu%2070,der%20Diagnose%20eine%20Remission%20erreichen
6 Northwestern University (2018): Rheumatoid arthritis meets precision medizine https://news.northwestern.edu/stories/2018/march/rheumatoid-arthritis-meets-precision-medicine/